
 |
 |
 |
 |
Basic Embryology
Spina Bifida
Related Issues of Early Development
Embryopathy
Fetopathy
Gills & Cranial Nerves
 |

Looking into the womb, we see the early small balloon-like bleb (in the womb, left; magnified view, center) attached to the womb lining. If we peel a bit of the roof from the balloon away (above right, below left and below middle) we see an oblong disk inside. It has a small groove at one end.

In the above far right frame is a representation of the general orientation of the disk, that is, basically which parts of the disk will become which parts of the developed person. The small pore at the left of the groove is an early pivotal development center, at the approximate location of the future low back. The overall disk is fairly simple at this point. Complexity of development increases as the different tissues begin to stream (move in patterns relative to each other) and cells from one place move up against other cells. This contact triggers interactions and further growth and development activity, and causes changes in the nature of the cells themselves - cells grow in number, but also in types.
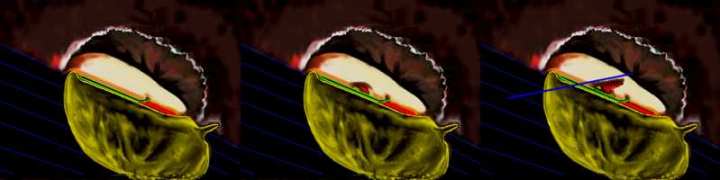
In a side view cross section showing only the embryo's right half, we see that that pore travels as a sinus within the disk toward the head end. The yolk sac is depicted as a yellow-green balloon-like hollow structure deep to the flat oblong disk. There are two fluid filled sacs separated by the disk, one above, and one below. The top side of the disk, the surface we first viewed, can be thought of as the "back side" since it becomes the person's back.
The yolk sac is on the future front or belly side. In the above left image we see a specialized tissue (in red) on the yolk-facing undersurface of the disk, right end (future foot end). This specialized tissue grows out and around the "notocord" (shown in green), and then fills into the space at about the middle / belly portion of the oblong disk, streaming in between the outer back surface (white) and the belly surface (yellow) around the sinus. The cut away pieces in above center and right views show stages in the progression of this middle invading layer (which is called the "mesoderm").
So, ectoderm (outer layer), mesoderm (middle layer) and endoderm (deep layer).
Ectoderm => skin & nervous system
Endoderm => guts and gut organs (liver etc).
Mesoderm => the rest. ...eh, more or less...

Back to the top surface of the oblong disc. It is what becomes the "ectoderm". The groove pictured in these views extends lengthwise, forming a central stripe all the way to the head end of the disc, (which overlies the region of the green notocord structure we saw before and which lies just deep to this surface stripe of cell change. This central lengthwise surface strip of ectoderm will become the nervous system. The rest of this layer, to the sides, becomes skin.
Think of the brain and spinal cord starting out as a stripe on a skunk's back. Somehow it needs to sink in deeper and get covered over. Growth does that as the tissues under the skin thicken and swell as the central stripe sinks in. But before that insinking is completed, the disk is getting centrally puffy, more so at the head end as the central area sinks deeper.
Remember the red tissue that invaded the middle of the disk and created the middle layer, called mesoderm? It becomes skeleton and muscle. The belly side layer becomes the digestive tract from mouth to anus, with all the organs that empty into that tract (liver, pancreas etc). The mesoderm organizes itself into transverse parallel segments. We see three such right-left pairs of segments in the above right image. Those lumpy mesoderm segments are called somites. The central swelling, bigger at the head end, is the early upper nervous system. The early brain begins as the two large swellings with the deep cleft between (middle and right images).

This process continues with more detail popping up at the head end and more length toward the tail end and lots more somite pairs. The parallel neurologic swellings are connected in an inwardly-bent U-shape, but notice in the above right frame that in the middle of the length that U-shape has sealed left to right in an O-shape. That coming together of left and right drags the skin tissue with it, resulting in the neurologic tissue being underneath the skin at those places where the U-shaped trough zippers closed in both directions (from the middle toward the head, and from the middle toward the tail).
Although the above pictures expose the somites, they are actually covered by skin. As the skin swells up to cover the newly formed "neural tube", like a wave rising to break over a pier, it carries the deeper middle layer (mesoderm) which is tiled in somites. That segmented mesoderm is carried up and over the neural tube as well. The neural tube reacts by sending branches out, left and right, between the somites - nerves.
Below, we see the brain is forming new lumps. The fore brain and mid brain are becoming distinct from the hindbrain. The image on the left has a cross section near the tail end which that the endoderm (yellow) is also getting more tube like in the process of forming the gut.

The definition of the brain gets more complex as the sulcus (central cleft) develops zones of space and eventually creates a left space and right space within the nerve tissue as the zipper process not only covers the brain with skin (and mesoderm - bone etc), but also as a septum develops as a wall between right and left brain sections. The first two ventricles of the brain flank this wall. As the two sides approximate, right to left and left to right bridging of nerve cells occurs above the ventricles.
This closing - tubulation - from middle embryo to head end and middle embryo to tail end - of skin and muscle-skeleton over the nervous system is a big deal. The coming together of right and left can in some cases be slowed in a subtle way so as to render a person broad faced. Width between the eyes is increased. Broad mouth. It can be overt as in cleft lip or cleft palette, neither of which involves a splitting but rather are cases when two sides did not join fast enough before skin covering formation overtook the joining process.
 When one sees the trait of slowed coming together of right
and left, one wonders how deep that slowing was. If very deep, we may have a failure to create that dividing wall of neural tissue, resulting in a large single central ventricle
rathet than right and left ventricles, or some degree of partial ventricle formation (there should be two in the forebrain, one in the mid-brain, one in the hind-brain).
When one sees the trait of slowed coming together of right
and left, one wonders how deep that slowing was. If very deep, we may have a failure to create that dividing wall of neural tissue, resulting in a large single central ventricle
rathet than right and left ventricles, or some degree of partial ventricle formation (there should be two in the forebrain, one in the mid-brain, one in the hind-brain).
The ventricles when formed properly connect with one another, very much like the Great Lakes. If the connections between them are misformed or become plugged, ventricle outflow is blocked, and they can swell
with excess fluid that is unable to drain (hydrocephalus).
The corpus callosum (the neural bridge which allows the left and right brain hemispheres to inter -communicate) may well fail be absent or deficient in part as a result of the slowed coming together. An enlarged hind brain ventricle, called a Dandy-Walker cyst, is another potential residual effect of slowed joining, it being not a growth as such but a failure to replace ventricle space with substance in the coming together. Cranial nerve and facial embryology are complex issues.
To put a relative value on this left-right joining processs (although these numbers vary according to
the kind of hospital), generally 90% of hospital admissions to comprehensive facilities relating to central nervous system anomalies are failures of the tube to zipper in some degree. A doctor in
England theorized, and was found correct, that certain vitamins were capable of reducing the failures. Stated the other way, vitamins may be able to prevent certain birth defects. Folate specifically was pointed out. Beware, ladies, we already
know that certain other vitamins in EXCESSIVE amounts can also cause birth defects. Nature isn't this or that, it is about balance. BALANCE.
prevent certain birth defects. Folate specifically was pointed out. Beware, ladies, we already
know that certain other vitamins in EXCESSIVE amounts can also cause birth defects. Nature isn't this or that, it is about balance. BALANCE.
But notice (on the right), a chemical called aminopterin, a substance used by experimenters which because of its similarity to folate can substitute itself for folate in the body, can cause the zippering process to fail. It can cause neural tube defects. It looks a whole bunch like (almost exactly like) folate! Look close, see the tiny difference? That is the key to poisons! "Almost like nature" is a deadly recipe. It fools nature into taking it in but then not only doesn't work but clogs the machinery. You are better off eating crushed bricks and asteroid fragments than some substance that is nearly like nature. Thalidomide was a close match to a natural substance. Close is trouble.
 The reality is that taking folic acid supplements does greatly
reduce neural tube defects such as spina bifida. Folate is
needed badly by rapidly dividing cells as it is a helper in the making of DNA, at the core of every cell. But it also helps certain other processes, including one that scavenges
metabolism by-products and enables the cells to dump the garbage. The cellular sawdust of the metabolic workshop has to be swept away.
The reality is that taking folic acid supplements does greatly
reduce neural tube defects such as spina bifida. Folate is
needed badly by rapidly dividing cells as it is a helper in the making of DNA, at the core of every cell. But it also helps certain other processes, including one that scavenges
metabolism by-products and enables the cells to dump the garbage. The cellular sawdust of the metabolic workshop has to be swept away.
Oddly, when you test women who have given birth to
babies with neural tube defects, they do NOT have a measurable folate deficiency - at least not as defined by current standards. Measured folate levels do not reflect the problem. However, all the
dietary guru's are saying "yah yah, told you so!", that the normal diet should include a higher level of folate. Maybe so, but it may be true for another reason: that the specific needs for a vitamin may
VARY from one person to another. The level of folate generally considered the proper level may, indeed, be the optimum for MOST women. However, some women may require a small EXCESS to offset some other problem unique to them. One such problem is xanthine
oxidase. In a circumstance wherein that enzyme is faulty, an excess of folate may offset the problem. Right now we know that raising the folate level in women by a certain amount is
safe and does overall reduce the incidence of birth defects. An obvious reason for caution is seen with other vitamins, such as vitamins A, D, and C, which if taken in excess can produce birth defects.
level may, indeed, be the optimum for MOST women. However, some women may require a small EXCESS to offset some other problem unique to them. One such problem is xanthine
oxidase. In a circumstance wherein that enzyme is faulty, an excess of folate may offset the problem. Right now we know that raising the folate level in women by a certain amount is
safe and does overall reduce the incidence of birth defects. An obvious reason for caution is seen with other vitamins, such as vitamins A, D, and C, which if taken in excess can produce birth defects.
The problem is that the folate is needed right up front. It is needed from day 1. By the time a
woman knows that she is pregnant, it is already too late! It is imperative that all women of child bearing age be child ready. Planned or otherwise, the cost of 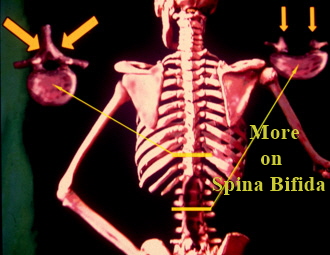 care of children with neural tube
defects, and other similar problems not discussed, is enormous.
care of children with neural tube
defects, and other similar problems not discussed, is enormous.
Left, we see the skeletal effects of failure to tubulate. The upper vertebral cross section is projected in the left inset. A spinal canal is fully enclosed in a bone tunnel. The lower incompletely tubulated area is projected in the right inset. Not only is the spinal canal bone roof missing, but the vertebral body is more shallow and splayed out. The failure in the neural tube formation also has prempted proper nerve cell formation and proper differentiation. It is not unusual to find islands of wrong tissues along the edges as the defect, where the stepwise unfolding of new tissues and tissue types can get lost. As the peripheral nerves come from the edge tissue, they may or may not succeed in getting formed. If so, there may be no connection to a functional spinal cord, and / or the neural elements (spinal cord precursor) way wind up being a large cystic structure containing odd tissue types. Occasionally small islands of spinal cord do form which are not connected to the rest of the neurologic structures. These islands of neurology generally behave as spastic circuits. You can distinguish them by their reactivity to lower limb stimulus but nothing else. They usually just make trouble.
Embryopathy:
Defects in the processes listed above, the basic separation of tissues, subdivision into zones for one organ versus another... any early primitive process failure is embryopathy. The embryo is the
precursor growing form in which tissue type differentiation is still occurring. Embryopathies are severe. The absence of one step will often botch subsequent steps of even seemingly unrelated
structures. That "notocord" mentioned earlier? That is what tells the mesoderm to make vertebrae. A defective notocord will cause a failure of spine formation, muscle formation, neurologic formation
, and leave behind such confused tissue as to create bizarre tumors which generate little human parts within them.. Normally, the mesoderm separates the ectoderm and endoderm. Allowing
ectoderm to touch endoderm causes a hole to form (this happens normally for the formation of the mouth and anus). Failure of the mesoderm to get out of the way allowing those two surfaces to
touch will cause a failure of a cascade of processes in the formation of the oral and rectal organs. If an organ is deficient from embryopathy, it isn't clear that there is even tissue that has capability of
being the organ in question. A hip failed at this stage may leave tissue in the hip area that has no idea of its own hip-ness. It may not even know joint-ness or hardness or whatever. Early
development is not just a shaping of clay. The tissues are becoming sequentially programmed for their later roles as organs. Left behind by some failed signal to read the next code, that tissue gets
genetically lost. It is not uncommon to see small islands of cells which got lost and which grow just winging it. A teratoma is a cyst in the body with skin like properties with hair and teeth growing. That's lost.
Fetopathy:
Once all the organs are built, and the issue at hand is primarily one of increasing size, the form is called a fetus. To get that far means that most of the blue prints are intact and most of the tissue
inducing signals were sent. Details may be lacking (for example, the fetus at this point is still more suited to the conditions inside the womb than to the outside world - those alterations for outside
existence may still not be activated).
There can also be external influences that cause problems. Deformations to the plastic fetus can be caused by being too tightly packed or in an awkward position in the womb. Often such shape disorders are either self-correcting or can be nudged back in line with minor intervention, and they will do well because the blue prints for structure are proper.
Example: the mild incurved foot common to so many babies is a fetopathy. The severe club foot is an embryopathy. The level of medical intervention for these two so-called "in-turned feet" is worlds apart.