
 |
 |
Gills
Development of the Cranial Nerves
Facial Relationships
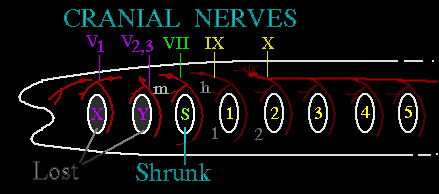
The very early phase of human embryologic development looks very much like the very early phases of other mammals. But too, that looks not too unlike the early development of lower animal forms. Here we see the jawless primitive scheme. There is a central hollow running the length (gut) and a series of side openings - gill slits. Between each gill slit is a myotome (or somite) - that is, a muscle & skeletal tissue arch. Those somites will develop the cartilage and bone to support the gill slits and the muscles to control their opening and closing. A blood vessel passes through each arch between the adjacent two gill openings. The vessel arch is numbered 1, 2, 3... as the slit behind it.
The gill arch labeled "m" is that of the maxilla. It, in the higher forms that develop jaws, contributes the lower jaw parts and muscles. The arch labeled 'h' is more variable as the gill slit labeled 'S' shrinks and displaces upward. The 'h' gill arch becomes the 'hyoid' (in the high throat) bone as the 's' gill sinks in to serve as an auditory canal. The higher animals with jaws seal over the gill slits here labeled as 'X' and 'Y' (not their real names). The forward arches abut without the slit openings but maintain the neural branch and vascular branch structure as if the slits were still there. The forward three lost gill structures will become the musculature and supportive structures of the eye.
The olfactory (smell) nerve and the optic (vision) nerve are less "nerves" in the sense of nerves as develop between the somites than direct brain tracts extended to the periphery.
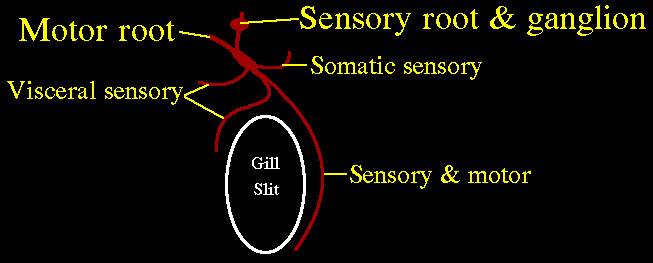
There is a general schema to the nerves relative to each gill slit. From the neural tube between each somite (at each arch) protrude two neural outreachings. One is "dorsal" (meaning on the back side of the neural tube) and one is "ventral" (meaning on the belly side of the neural tube). The dorsal roots are sensory and carry information to the neural tube (later brain and spinal cord) entering from the side but more to the back side.
The ventral roots exit the neural tube from the side more toward the belly side. The dorsal coming and ventral going roots join as a two lane highway outside the neural tube (later brain and spinal cord). The common mixed nerve travels to about the destination and splits up again to serve various needs. The forward branch serves visceral (gut and inner mouth) structures. The rearward branch stays mixed and serves skeleton and muscle (which require both sensory and motor components). Another rearward branch that comes off early, goes to surface sensation (somatic sensory).
Thus we see the overall scheme of parallel stripes of innervation, segment by segment, with nerves traveling between the segments. These patterns get drawn out into long semi spiral stripes when the arms and legs begin to protrude and drag their involved segments along.
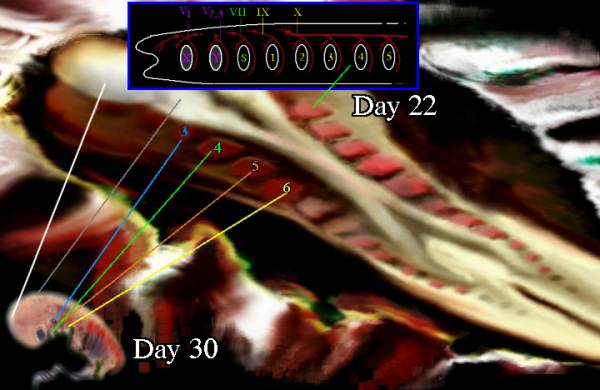 |
The very primitive scheme of the higher animals (in general) is more or less hard to discern in the most forward segments as the very high specialization early dominates and smudges the primitive details. Yet the relationships hold in that, when an arch goes bad, those things expected to be derived from that arch go bad together. There will be correlation of nerve abnormality with circulation abnormality and facial appearance. As several important glands develop from certain arches, certain neurologic oddities will correlate to certain hormonal defects. Thus the characteristic facial look of the child absent the parathyroids etc.
|
So, the Cranial Nerves are derived as follows:
I. Olfactory - a special direct brain sensory tract
II. Optic - also a special direct brain sensory tract
III. Oculomotor - mixed dorsal root 1 (autonomic) & somatic motor ventral root 1
IV. Trochlear - Somatic motor, ventral root 2
V. Trigeminal ("three part") - general somatic sensory V1,V2 &3,
special visceral motor V2, V3
VI. Abducens - ventral motor root 3
VII. Facial - Some of everything sensory, autonomic (visceral motor). No somatic motor.
VIII. Auditory - another special direct brain sensory tract
IX. Glossopharyngeal - Some of everything sensory, autonomic.
X. Vagus - All the visceral components.
XI. Accessory - same as X.
XII. Hypoglossal - Somatic motor, ventral root 5
These root counts are from the primitive scheme. To number them relative to human arches (which are lacking in the first 3). Thus the 5th cranial nerve is not a 5th arch nerve.
I. Olfactory - smell
II. Optic - vision
III. Oculomotor - four eye muscles from the original first cranial somite:
superior rectus, anterior rectus, inferior rectus, inferior oblique
ciliary body & iris
IV. Trochlear - fibers run anterior within the brain, cross within the brain to opposite side
then exit to eye superior oblique (from second cranial somite)
V. Trigeminal ("three part") - the jaw
VI. Abducens - eye posterior rectus muscle also from the third cranial somite.
VII. Facial - muscles of hyoid arch which develop into facial muscles
VIII. Auditory - hearing
IX. Glossopharyngeal - throat and larynx muscle, sensation and some taste, salivary
X. Vagus - visceral sensation, parasympatheticpathway,
XI. Accessory - similar to X.
XII. Hypoglossal - tongue motor & some pharynx
Note III, IV, VI, & XII are very similar and akin to the ventral motor spinal roots.
One important immediate application of this information, in a general way, is in the distinction between neurologic impairment due to nerve trauma (mechanical damage after the fact) - and embryologic formation failure. Formation failures will be anatomically sequential and of like embryological kind - gill by gill, somite by somite (say... those things derived from upper portions of the forward parts of gill arches and somites).
Trauma induced failures will be geometrically clustered or along lines of force. So, a child with a brachial plexus palsy with unusual sparing of sensation and - oh by the way - some facial assymmetry and a smaller calf muscle in the leg on the same side.... bells should be going off. So should the youngster be going off to get some ultrasound of certain organs.
 |