
 |
 |
 |
 |
 |
Spina Bifida
If ever there were a topic difficult to extract from a pure discussion of embryology, this is it. You may wish to read that section first, as we will not dwell on cause, here. This section is aimed at getting a perspective on the subject.
In the most characteristic case, the skeleton spine formation is incomplete in the back to the degree that the spinal cord is not only exposed but extruded outside the body in a sac of covering tissue. That mass protruding from the low back is cystic (cyst = 'cele'). The nerve elements (myelo as in myelin is the nerve portion) might be intact, partially disrupted, or totally lost as a developed tissue. A myelocele is a bulge with nerve in it. If the spinal cord itself is intact and only the spinal cord coverings (meninges) are extruded outside then the sac is only a sac of meningal tissue with fluid. That is a meningocele.
If only the bones are defective and the spinal cord and its miningeal coverings are intact, and the skin is also intact, then the spina bifida (open spine) isn't open but rather occult (spina bifida occulta).
If the incompletely infolded tissues get so developmentally lost as to not know what they are supposed to be, they often guess, and guess badly. We may see streaks of inappropriate vascular dense tissue (hemangioma) or growth of odd fibrous and fatty tissue (fibrolipoma) or even find islands of inappropriately specialized tissue (kidney etc).
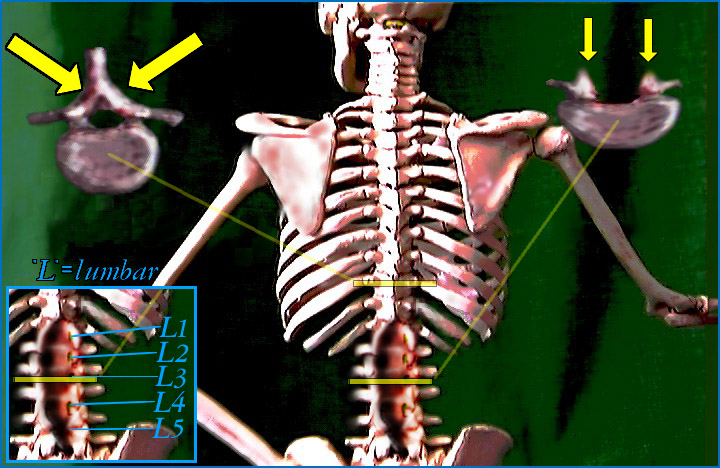
In the lower spine area which infolds last, defects are often extreme. Interestingly, spina bifida in the upper spine (where the embryologic infolding begins) is less often severe. There, it often does not involve nerve tissue or when it does, it does so less completely. Therefore thoracic involvement is usually meningocele, coverings bulged without spinal cord involvement, and not myelomeningocele, the whole megilla.
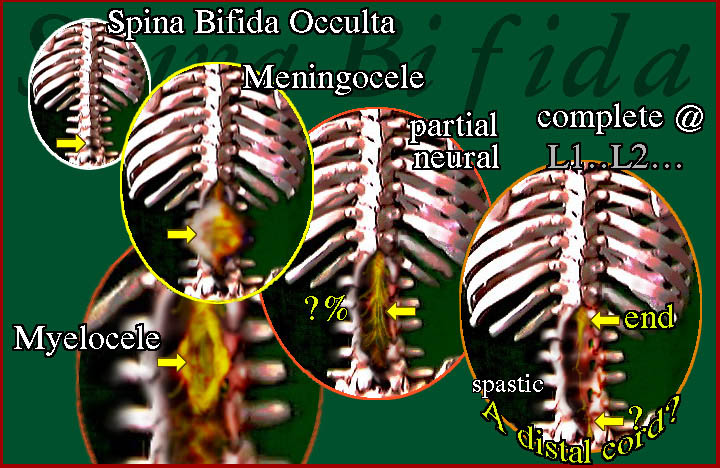 |
Here we see the spectrum from the least type (occulta, which occurs in 5% of the population) which usually goes unnoticed unless an x-ray is taken for other reasons. The meningocele - if purely such - might have no neurologic deficits at all. The issue is one of prevention of infection with secondary damage to the nervous system. Removal of the excess sac and coverage with skin is the usual treatment. There may be partial nerve oddities or the spinal cord may be confused in its formation as a cyst (myelocele) of nerve tissue that has no or some useful functioning portions. In the extreme cases, whole sections of spinal cord may be missing. It is possible to have a piece of spinal cord formed beyond the bad area. If so, lacking connection to the rest of the nervous system, it will behave as a spastic driver of whatever it innervates.
The failure to form a complete neural tube can involve the brain and the skull in a severe way leaving a protruding sac off the head (encephalocele) or can manifest in lesser ways as described below.
Why?
 |
The causes are many. Slowed production of DNA sub units can render the folding of the nerve tube incomplete, leaving a cross section that is U shaped rather than O shaped. About 75% of fetal deaths are related to this, more or less. There seem to be predispositions that suggest a single gene defect in a small percentage of families. But more cases result from several genes not working well when paired with certain other genes.
 |
Anencephaly = total absence of the brain. Encephalocele = partial deficient development of the brain with an external cyst. Enlarged ventricles may be caused by fluid retention, but also may represent an incomplete tubulation. Such enlargement of the fourth ventricle is a Dandy Walker "Cyst". That cyst implies that infolding was incomplete and therefore that other structures that depend on infolding may also be abnormal. Dandy Walker cysts are often paired with incomplete corpus callosum formation (that links right and left brain), or with forebrain septal defects (wherein hypothalmus gland regulating, hunger thirst regulating, and neuroendocrine regulators reside). Wide distance between the eyes is also an aftermath of slowed joining of left and right sides.
The genetics are odd in that the predisposition to have a child with spina bifida is more likely to follow generations of women. That faulty tubulation follows maternal lines more so than male raises questions about the DNA in mitochondria (the power makers of the cell) passed on by the mother only or the mother's chemistry as a milieu for the fetal development. Because it is multifactorial, no one formula can be applied without study to a specific case.
 |
One thing is for sure, certain vitamins (Folate specifically) can reduce the incidence of this catastrophe . The problem is that by the time a woman knows that she is pregnant, the defect is already a done deal! Young women must be kept healthy at all times, period. By the way, fun seekers, this applies to many other fetal issues as well. Cigarettes, booze, starvation states all damage babies at the onset.
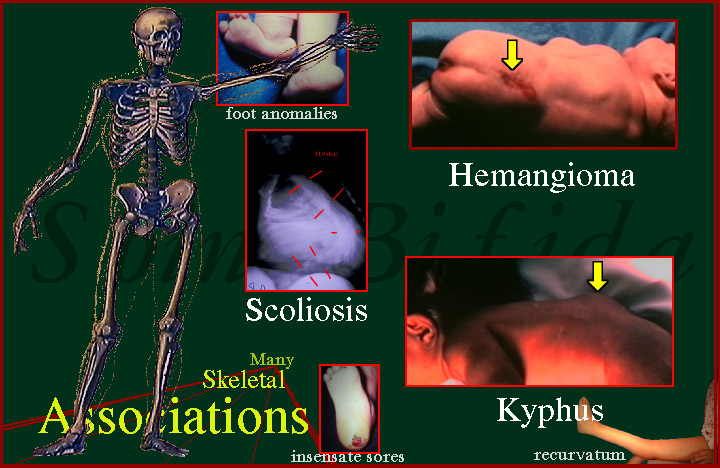 |
There are so many associated problems when spina bifida is present. These are not just the ill formed shapes of structures, but how they behave and fail even further with time. Hips that are socketed at birth can and do pop out, knees can and do bend in wrong directions (brace protection of knees is so very important). Skin lacking sensation breaks down. We have seen deep thigh ulcers from a steering wheel pressing the thigh (seat was up too high). Without sensation, such a simple thing becomes a long hospitalization outcome.
 |
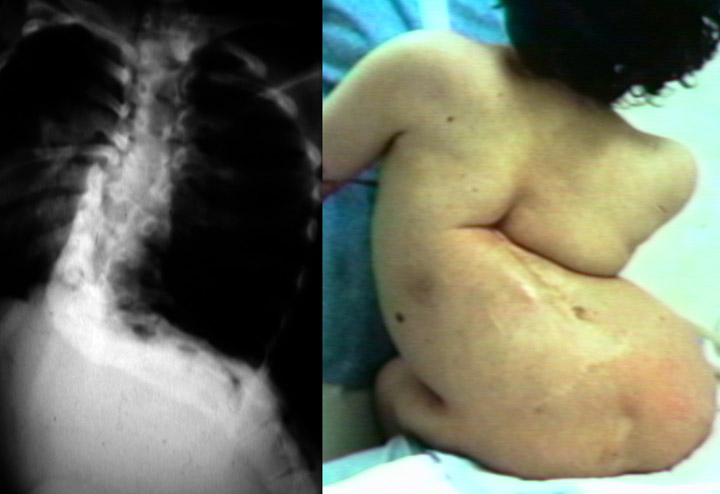 |
Spinal deformity may be severe beyond belief. See the scoliosis section for more on how we deal with this.
The degree of problem has much to do with how much neurologic structure is missing. This is in two forms. How much sensation is lost? How many muscles are without enervation?
We discuss the LEVEL of spina bifida, however by stating what is left INTACT. So if L5 nerves are gone, then the child is said to have an L4 Level. That would be too easy. When we are dealing with new borns, we can't ask them to do this act or that move and expect to learn anything. For that reason, in babies, the LEVEL is the level of intact SENSATION. Why? Babies react just fine to getting flicked, or poked - if they feel it.
Older children are described by their motor level, as that better correlates with what they can do. But, remember, muscles with good innervation are poorly coordinated if sensation is lacking. A child with spina bifida with far more intact muscle than a child with polio will not perform as well as the child with polio. Why? Polio spares sensation.Sensation guides muscle movement and is essential to the biofeedback involved in compensatory movement mechanisms.
The two kinds of "LEVELS":
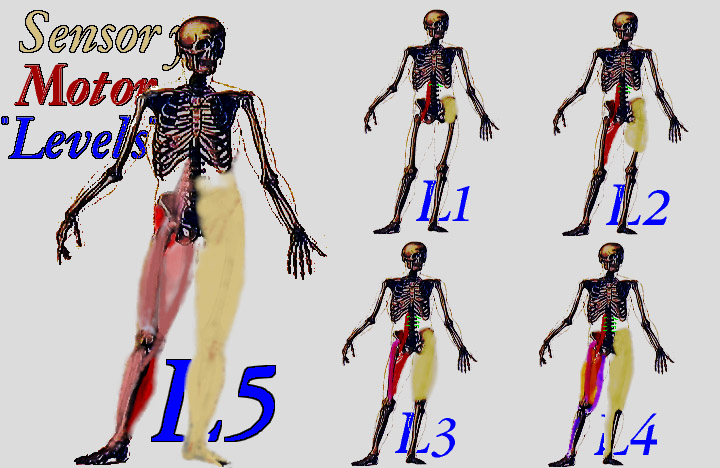 |
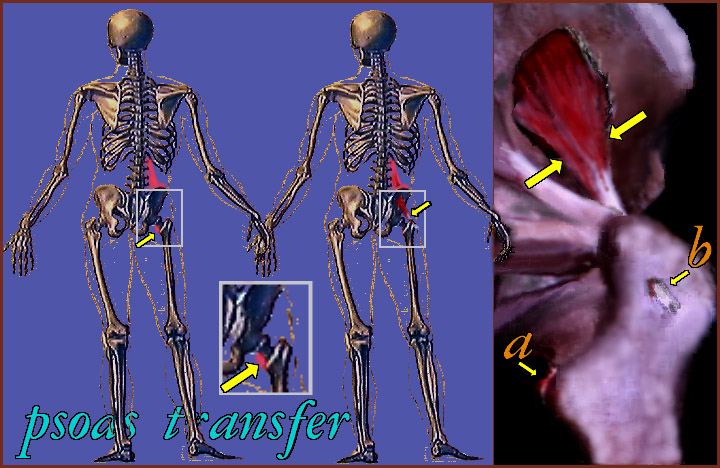
On the skeleton's right side (our left) we see the muscles that are working. On the opposite side is depicted the skin of the leg region that has sensation intact.
In an L5 level, (large image on the left) most muscles are intact except for some small muscles inside the foot and most sensation is intact except sensation between the 1st and 2nd toes.
Note that L1 level, has only some hip flexor muscle innervated. That flexor happens to turn the leg outward as well as flex the hip. A baby with an L1 level will be at rest with the leg flexed at the hip and outward rotated - so we do get some idea of motors in new borns.
The other levels (L1, L2, L3, L4) are as depicted above.
Let's look at one example in detail:
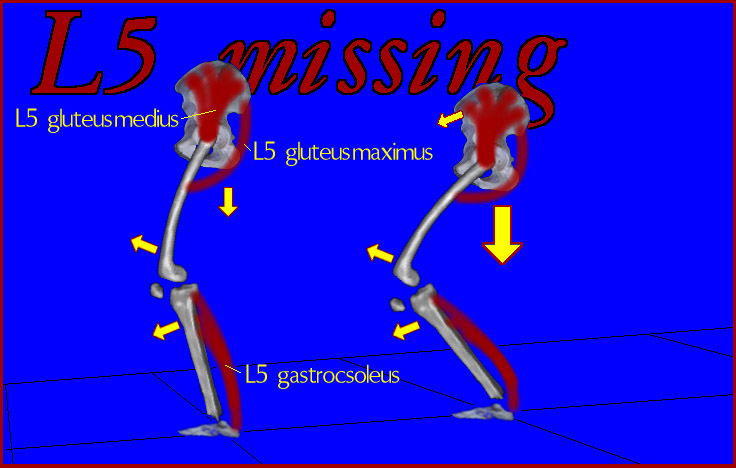 |
With an L4 level (L5 missing), we lack important antigravity muscles: The gluteus medius (hip abductor), the gluteus maximus (hip extensor and outward rotation), and the calf group of muscles (gastrocnemius and soleus) which push the foot against the floor. Only the quadriceps (front of thigh) can extend - but it will need help. Additionally, inability to straighten by way of weakness may be worsened by development of contractures (undergrown structurally short muscles) favoring the flexed posture. Indeed, those contractures may constrain posture to only flexed positions. Then what?
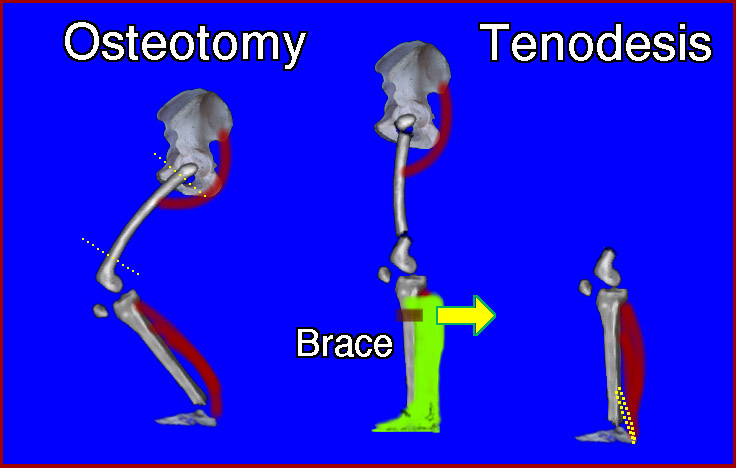 |
A solid ankle brace at the foot provides important protection against over flexion. Hinges here, are simply the result of improper knowledge. Surgical methods may be used to 1) undo fixed contracture and 2) provide some static stability by attaining a balanced posture which requires little muscle effort. We see, in the middle image, where the knee joint has been surgically rotated and the hip divided and reset straighter so as to allow standing. The right image shows how the foot can be stabilized internally . Freedom from contracture is so important that it is better to be straight with dislocation of the hip than bent with hips intact. Without power, there is no way to maintain erect posture if the starting posture is flexed.
 |
In the early days of spina bifida treatment, it was assumed that the hips just HAD to be kept in the sockets, even though it is so hard to keep them there. Very complex surgeries were designed to put muscle in the position of the gluteus medius (hip abductor) because that muscle keeps hips in - somewhat. But the trade off was loss of a forward motor. We now do this rarely. The trade wasn't worth it. Spina bifida patients with good posture and dislocated hips do far better than those with flexed posture and intact hips.
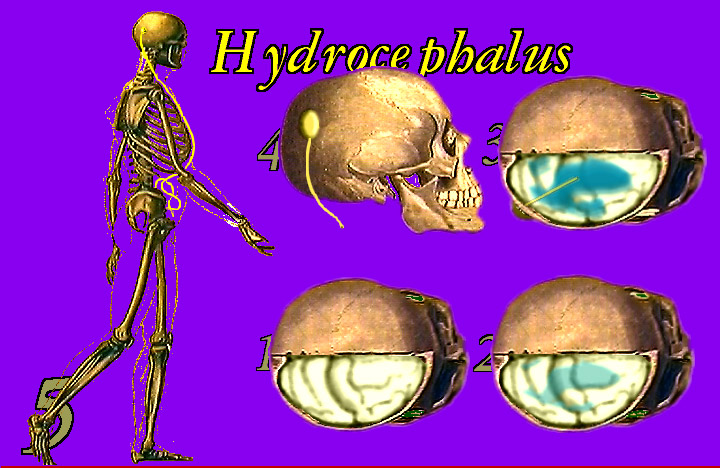 |
 Hydrocephalus. 1. Inside the skull is the brain. 2) Inside the brain is an internal series of cavities - interconnected lakes of fluid - the ventricles. The brain forms the fluid which runs from
one lake to the next (like the Great Lakes issuing toward the sea) toward the outer surface. 3) When the outflow gets blocked, the lakes swell with fluid and, in a baby whose skull bones are
not yet interconnected, the skull swells to accommodate. The brain thins over the enlarging ventricle lakes (hydrocephalus). 3) A thin straw (shunt) into one such
lake (or more) can allow that fluid to be vented. Simply bypassing the obstruction does not work as it gets plugged again. 4) A one way flow valve on the skull and tubing into the ventricle(s) vents the
flow to places that tend not to obstruct. The most common place is the 5) abdominal cavity (not in the intestines but in with the intestines). The other place is the heart by way of a vein. There are complex
reasons why one is used in certain circumstances over the other.
Hydrocephalus. 1. Inside the skull is the brain. 2) Inside the brain is an internal series of cavities - interconnected lakes of fluid - the ventricles. The brain forms the fluid which runs from
one lake to the next (like the Great Lakes issuing toward the sea) toward the outer surface. 3) When the outflow gets blocked, the lakes swell with fluid and, in a baby whose skull bones are
not yet interconnected, the skull swells to accommodate. The brain thins over the enlarging ventricle lakes (hydrocephalus). 3) A thin straw (shunt) into one such
lake (or more) can allow that fluid to be vented. Simply bypassing the obstruction does not work as it gets plugged again. 4) A one way flow valve on the skull and tubing into the ventricle(s) vents the
flow to places that tend not to obstruct. The most common place is the 5) abdominal cavity (not in the intestines but in with the intestines). The other place is the heart by way of a vein. There are complex
reasons why one is used in certain circumstances over the other.
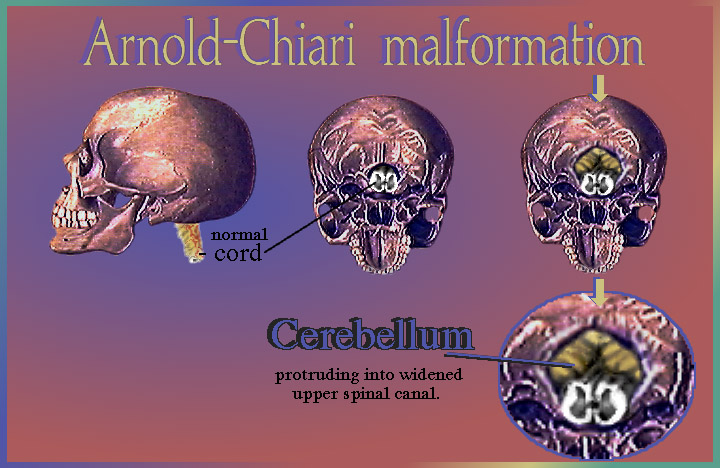 |
As we noted before, the tubulation begins in the middle of the spinal region of the embryo and zippers closed from center up and center down. Therefore, in spina bifida, defects in spinal tubulation may be shared, even though to lesser degree, by the upper spine and base of skull. Although it is not open in most cases, the topmost spinal canal and entry into the skull may be large - too large. The hind part of the brain may droop into the upper spinal canal through the over sized opening into the spinal canal. The cerebellum, doing the drooping, may pinch certain nerves in this location. The result is voice change - to a nasal quality. The word "egg" when spoken sounds like "eng". There may be gagging as the pharynx (upper throat and palate area) becomes uncoordinated. This is a very dangerous circumstance.
 |
Brain Interactive Model
Latex. About 25% of persons with spina bifida have sensitivity to latex. It can be lethal in even tiny exposures. Toys with latex are to be avoided (Koosh balls, balloons etc.). The sensitivity may weakly cross react with bananas or macadamia nuts. Operating rooms must make special provisions for all persons with spina bifida, just to be safe.
So, of all this stuff, what do you suppose persons with spina bifida are MOST concerned about? [We, The New Jersey Spina Bifida Assn., did a comprehensive survey of things that are of potential concern. Lots of questions to fill a pamphlet., even shopping and price questions.]
 |
This.
Seriously. No, not baseball! Socialization. And the most limiting fear in this regard? Looking different? Speed getting around? What?
 |
Incontinence.
In fact, the lethal issues barely got notice. Bones - nobody cared. Sores? Ehh. The only driving concern is continence, of bowel and bladder. These limit ease of mind in school and at work.
 |
This is how incontinence is viewed by persons with spina bifida.
The general surgeons and urologists are on it. It turns out that the appendix has good uses just waiting.
Medically, the most day to day essential area of concern is kidney function. Regular urologic exam is
absolutely vital. We still see, in our orthopedic setting, persons seeking some foot fix who have no idea that they have almost no kidney function left.