|
The Elbow
The elbow is a region and the elbow is a joint. As a joint it is made up of more than one bone. There is the humerus, in the 'arm' (did you know that arm means upper arm?). There are the ulna, and the radius bones in the forearm.
Yup, that's three.
|
|
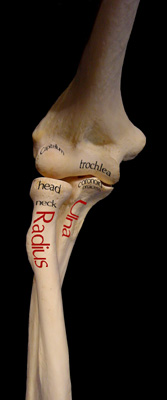 The elbow might be better called the elbows as there are two very distinct joints with
different agenda. The lesser joint is that between radius and capitellum. That is the joint which is a pivot for forearm pronation (palm down) and supination (palm up as in holding soup). The elbow might be better called the elbows as there are two very distinct joints with
different agenda. The lesser joint is that between radius and capitellum. That is the joint which is a pivot for forearm pronation (palm down) and supination (palm up as in holding soup).
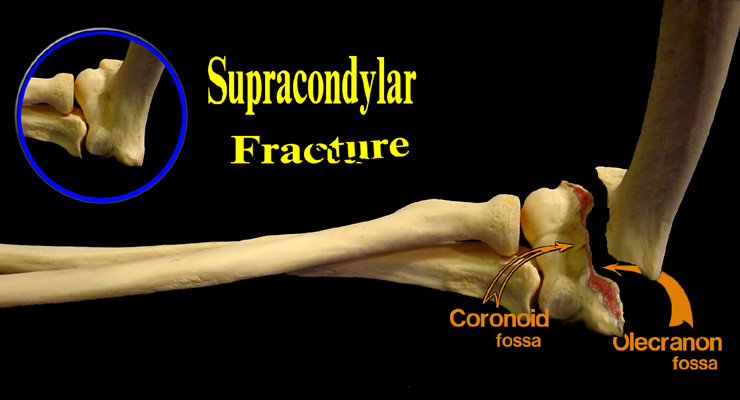
The other joint is that between the trochlea and the olecranon portion of the ulna. The ulna,
at the elbow, is F- shaped. The top of the F is the olecranon. The short piece is the coronoid process. When the elbow flexes, the coronoid process tucks into a hollow in the front of the humerus just above the trochlea.
The upper end of the ulna (the olecranon) tucks into a fossa (groove or hollow) in the back of the humerus when the elbow is extended (straightened).
Those two hollows - one behind, one in front - together make for a very thin bone. The humerus is thick on the
side edges but knife thin in the center area where these two hollows nestle together in a staggered array. This is where fractures are apt to occur. A horizontal fracture
just above the condyles through this thin central zone is called a supracondylar fracture.
The typical fracture drives the joint backwards such that the sharp lower edge of the rest of the humerus thrusts
forward. Nerve and artery damage can occur. For example one of the more common nerve injuries is a stretch of a
branch of the median nerve (median nerve is at ground zero for this fracture) which supplies thumb and index finger
grip power. Fortunately that injury self repairs in most cases. Artery injury is another matter. Distortion of veins can
impede return blood flow and thus block arterial flow as pressure backs up. These are true emergencies - the blood flow, not the nerve nor the fracture itself.
Ideally we 'fix' (short for 'fixate' = to join together) these fractures with cross pins in one configuration or another
depending on the way it wants to fall apart. A typical pin pattern is seen on the right, but with the fracture a bit apart for clarity. The fracture would actually be together when pinned.
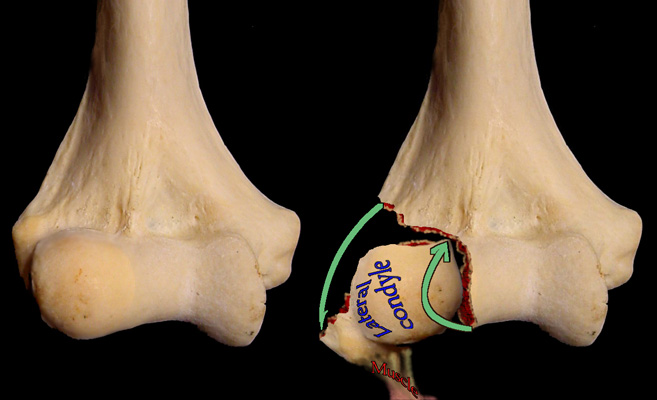
A lateral condyle fracture is particularly pesky as it typically fractures into the joint. It may well miss or split the
trochlea. The disruption of the joint surface makes repair mandatory. The wrist and finger extensor muscle
attachment tends to not only pull the fracture apart, but also tends to flip it over. These cannot be nudged back
through closed skin but require open surgery to control the flip, the spin, the roll and the joint line surface integrity. How these are pinned depends much on the shape of the fracture hunk and how it wants to displace.
|