 |
Kyphosis is often a secondary posture which merely sits on a lower back lordosis. Typical 'slumping' posture is more often than not caused by lax abdominal muscles allowing a sag into lumbar lordosis.
When the lumbar spine arcs forward, the spine above must do the reverse or else the face will be looking at the sky or the individual will be falling over backward. Every zig needs a zag.
 Of course, merely actively bending forward produces more kyphosis. The lumbar lordosis either flattens or rounds into kyphosis
depending on flexibility.
Of course, merely actively bending forward produces more kyphosis. The lumbar lordosis either flattens or rounds into kyphosis
depending on flexibility.
But pathologic kyphosis isn't about flexibility. The  serious forms have rigidity as a factor. Nobody is intentionally bending. Again,
we are talking about a process, not just a shape.
serious forms have rigidity as a factor. Nobody is intentionally bending. Again,
we are talking about a process, not just a shape.
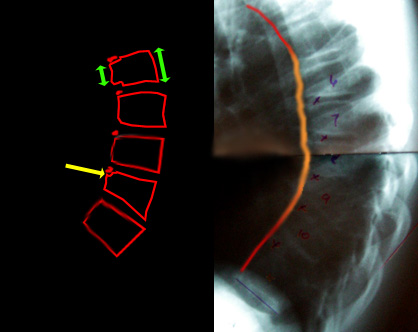
In a condition called Scheuermann's Disease or Scheuermann's Kyphosis, the curvature can be prominent and enhance with forward bending. But it is considered
more serious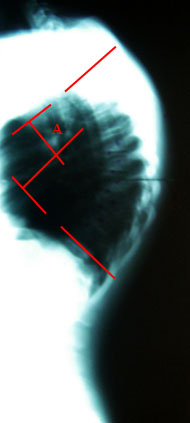
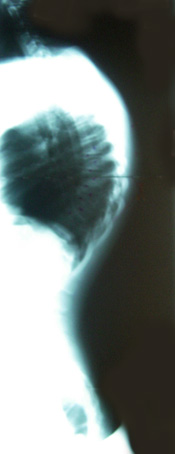 when it cannot straighten to near normal when bending
backward. A sideways x-ray taken with the youngster lying supine (belly up) with a small rolled towel under the most prominent center of the kyphosis tells us just how nasty it is.
when it cannot straighten to near normal when bending
backward. A sideways x-ray taken with the youngster lying supine (belly up) with a small rolled towel under the most prominent center of the kyphosis tells us just how nasty it is.
A general angular limit of 50 degrees (A) sets the limits of casual consideration. Of course the younger the patient (with more time for a kyphosing PROCESS to get into big numbers) the more that matters.
 And what is that process?
And what is that process?
We don't know.
Aha, but we have theories. We always have those. The one I like because it fits every other theory (whether it is the correct theory or not) is the one that notes that there is a single long ligament - the anterior spinal longitudinal ligament - which runs - guess.... yes the length of the spine on the anterior surface. If that ligament, for some magical reason, has a span which just won't grow, then the front of the spine would have a fixed length as the rest grew and curved into kyphosis around that limit.
We see the vertebral bodies short in front and bigger in back (wedged). The growth cartilage rings look unhappy on the front edges of the involved vertebrae. We see fragmented bone formation in the scooped out nibbles of the vertebral front edges which are actually delayed bone areas filled with cartilage.
Exercise!! Yeah, right. Just about every nice health sounding word gets tossed at this. Doesn't work.
A nice, firm but comfortable brace is a costly waste of time. With these buggers you really have to push.
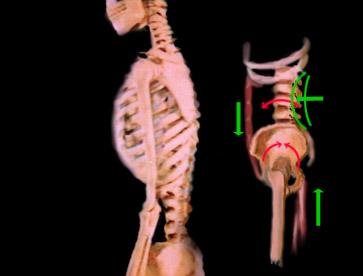
 This is a cantilever brace ( a cantilever TLSO). It is brutal but it can reverse SOME cases.
This is a cantilever brace ( a cantilever TLSO). It is brutal but it can reverse SOME cases.
The red star * is a pivot. Straps at the bottom apply really strong rotatory force to pads just at and below the collar bones. The rear of the brace is open above but firmly counter padded at the vertical red line.
As with all spinal deformity, correction depends on growth. Without growth, things, even if they do budge, will just spring back.
Many cases go untreated and just supply us with variety of the human frame in populations. As long as the process stops within reasonable limits the effects are not too bad. But some go on and on.
 This is an even more serious kyphosis. When the kyphosis is all within a single vertebra or pair, we call that sharp kyphosis a gibbous.
This is an even more serious kyphosis. When the kyphosis is all within a single vertebra or pair, we call that sharp kyphosis a gibbous.
This gibbous is in a toddler. These can go on to angle so severely so as to cause paralysis. In this case we see a deficiency of the entire front of one vertebral body on x-ray. Here, by MRI, we see the x-ray hole as being made of stuff. That stuff is aborted fibrous cartilage tissue. There were x-rays showing this thing getting more angulated. What do you do?
Stop it.
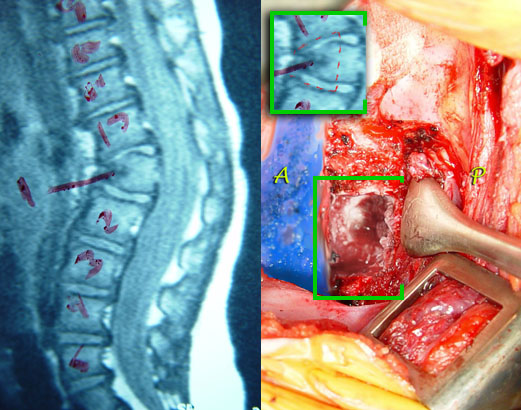 |
First the disturbed tissue is removed. But that is NOT what causes the process of further curvature. The progression of kyphosis is caused by the intact portions of the growth plates above and below which are unbalanced. After the disturbed tissue is resected, then the above and below hemi-growth plates are removed as well. We restore the normal contour with a transplanted bone secured with hardware. In essence bone will span this new single unit of once three vertebrae.
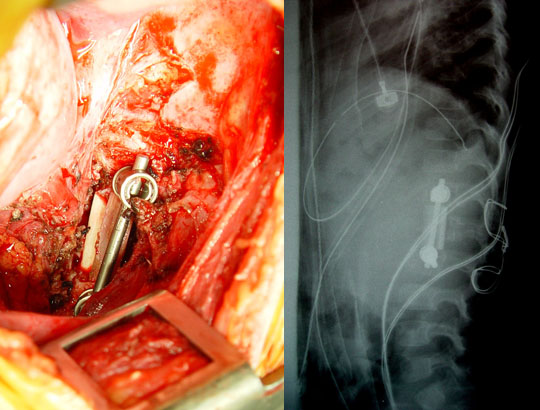 |
We see, above, a wire on the back side where small bone slivers are placed to fuse this same segment from the rear. The x-ray shows the contour restored.
The gibbus or sharp kyphosis is gone, but more importantly, the process which produces it is also annulled.
 Then there is this. Similar in appearance, but even more ominous than the growth defect above is collapse of vertebra from spinal tuberculosis.
Then there is this. Similar in appearance, but even more ominous than the growth defect above is collapse of vertebra from spinal tuberculosis.
There is a group out there in ya-ya land espousing the better healthfulness of natural milk. Natural sounds so... uh .. natural, doesn't it?
Why, yes, it does. And what could be more natural than tuberculosis from cows? Why bother with Pasteurized milk with a few vitamins slightly diminished? Hmmm? Why?
 Tuberculosis from cows? Well, OK. That works for me.
Tuberculosis from cows? Well, OK. That works for me.
Dr. Eduardo Luque of Mexico saddled with many such cases had to secure the spine more firmly than the simple rods of scoliosis surgery at that time allowed. Borrowing the graft looping technique used in neurosurgery he implemented segmental spinal fixation with twist wires looped through the posterior elements of the spine and around paired rods. It is a method which, with many improvements, is still used for serious spinal reconstruction. It is also often also used in combination with newer methods.
 When confronted with true kyphosis in cases of scoliosis (see Scoliosis example 4), opening and restoring
the space anteriorly in the scoliotic spine which is narrowed can be performed. Here, disc structures are removed in their entirety. This creates flexibility to allow nasty scoliosis curves to be better
corrected. But narrowing
When confronted with true kyphosis in cases of scoliosis (see Scoliosis example 4), opening and restoring
the space anteriorly in the scoliotic spine which is narrowed can be performed. Here, disc structures are removed in their entirety. This creates flexibility to allow nasty scoliosis curves to be better
corrected. But narrowing 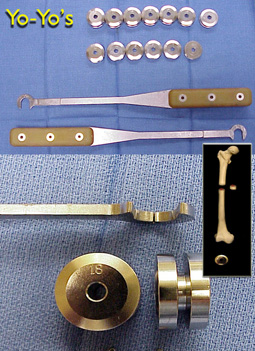 will aggravate kyphosis.
will aggravate kyphosis.
Yo-yo spacers are placed in the disc spaces to test contour.  They, having a variety of thickness and angular shapes, then serve as jigs
to shape bone grafts which then replace them. Metal fixation secures the contour. Bone healing replaces the grafted bone with native new bone.
They, having a variety of thickness and angular shapes, then serve as jigs
to shape bone grafts which then replace them. Metal fixation secures the contour. Bone healing replaces the grafted bone with native new bone.


