|
|
||||||||||||||||||||

 |
|
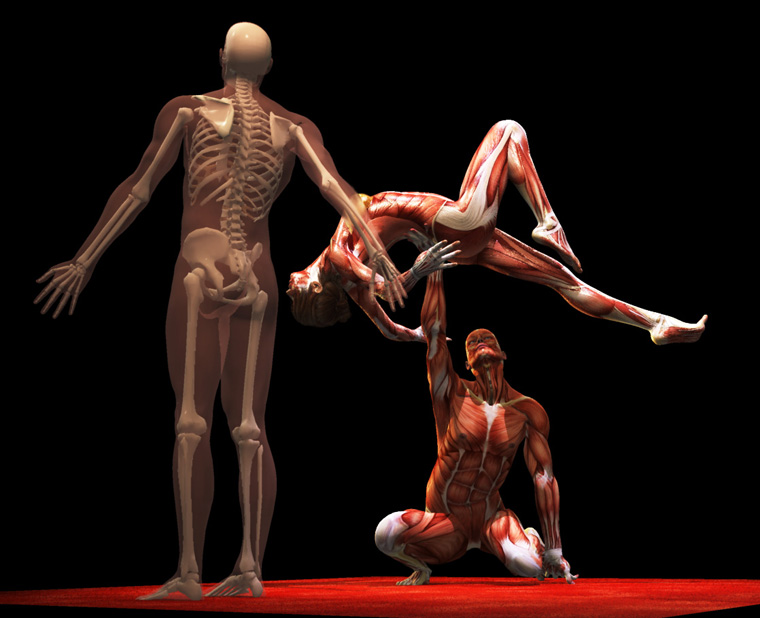
Did you ever wonder why gymnastics never caught on as a real professional sport? Whoa. Don't go off on me. Sure, it is seen in dance and circus everything but as an adult pro sport? No. Somehow the public has a problem with it. I know what it is.
Should I tell?
No. It's a secret. Secret hidden inside the brackets. Only special people may look.... by highlighting... [ It is all Isaac Newton's fault!!!! All that physics and stuff. You see, gymnastics has a set of rules - yeah, arbitrary but nobody wants to budge on them - so rules they are which define what is a good spin and what is a good landing and how a turn or roll should look. And physics (darn that Newton) demands that bodies spin on their centers of mass. So we have these rules which give big points to people whose ability to spin and flip and do physics-ical stuff does so on a friendly center of mass. That - my dear folks is a child-like center of mass. It moves as you mature to the place you see above, a nice place graceful in dance. Babies are all body and no legs. Body stops growing but legs keep elongating as we mature. So? They have a much different center of mass and so spin on a child-like center. Just as those beautifully trained kids get really skilled at gymnastics, their center of mass rug gets pulled out from under them. Gymnastics is - for most folks - not one of those SPORTS that you can carry intact into maturity for this reason. Old and out at 13 years? Hey, Isaac, that's not fair! So in an environment that respects the adult body form, dance, those skills carry over. To be an Olympian, however, you need a stunted growth disorder. You have to be or look like a kid ]
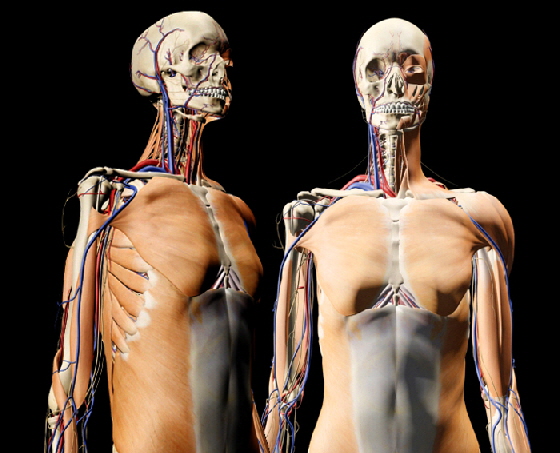
At full height our arm span exactly equals our standing height.
Nice and straight ?
Making someone straight as a surgical goal misses the fact that 1) nothing is straight normally, especially at the key moments some surgeons claim to seek it and 2) there are no 'right' angles (90 deg) in the human body. The phrase nice and straight refers, medically, to something make believe.
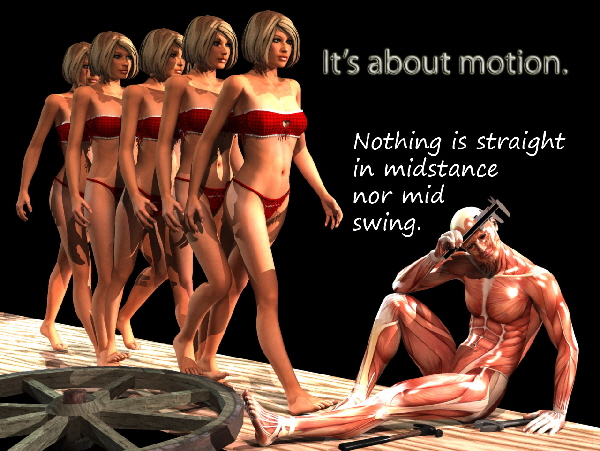
This image freeze is for his left and her right, midswing. It is also for the other legs, midstance. NOTHING is straight! Not supposed to be. To be straight here is to be stuck. On stop action video it is a sure sign of huge energy loss as deceleration is a part of the 'straightness' pathology.
At mid stance the ankle is NOT at 90 degrees! It is slightly dorsiflexed. That degree of dorsiflexion stays frozen all the way into swing phase and through swing phase. The the plantar flexion that does occur is part of a cushion at heel strike. If you supply a shoe heel cushion then nonmoving at slight dorsiflexion works just fine. A stuck foot in mild dorsiflexion will not be noticed but a foot mobile in plantar flexion (can't get past 90 to mild dorsi) will have you hobbling all over the place.
This smooth and narrow (side to side) transfer requires good feedback and intact sensation. When you see one side staying whole foot flat to the floor until the other is weighted fully you KNOW there is a sensory issue. The absence of the 'wheel' is the dynamic hallmark of even mild sensory loss. Oh, and the people who have this often do get 'nice and straight' looking for a wall to touch. One more relationship that is not obvious to beginners:
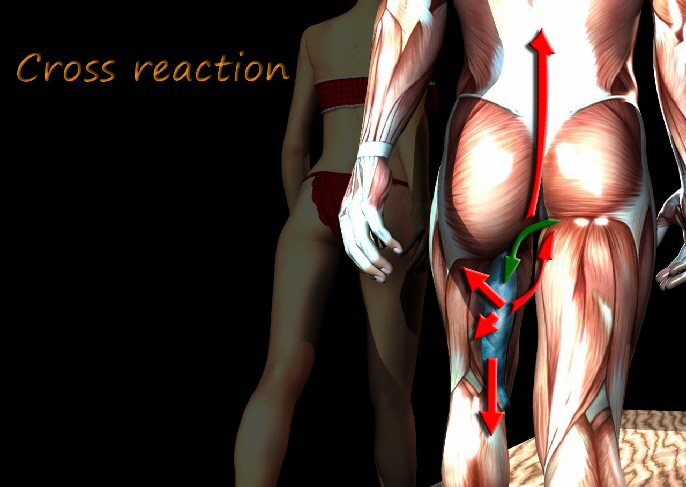
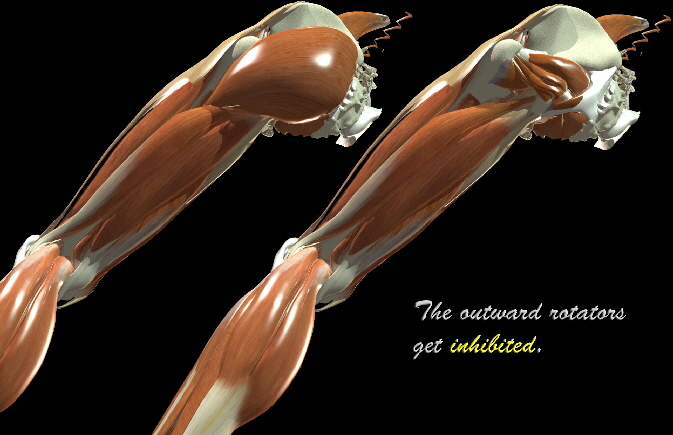
This is one of the hardest things to tack down in examination and you often have to slap yourself out of what you are already thinking to grab hold of this. To help you think of that wake up slap, remember that small rotational deviations are usually from too much something or from fibrosis limiting muscle. Severe malrotation nearly always has loss of opposition on top of more obvious deviation. Important? You bet. Severe medial leg rotation implies absent outward rotation and that means gluteus maximus is NOT working. At least some of the crouch may be unresponsive gluteus maximus action. That has a whole different everything behind it treatment.
|
||||||||||
|
|
||||||||||
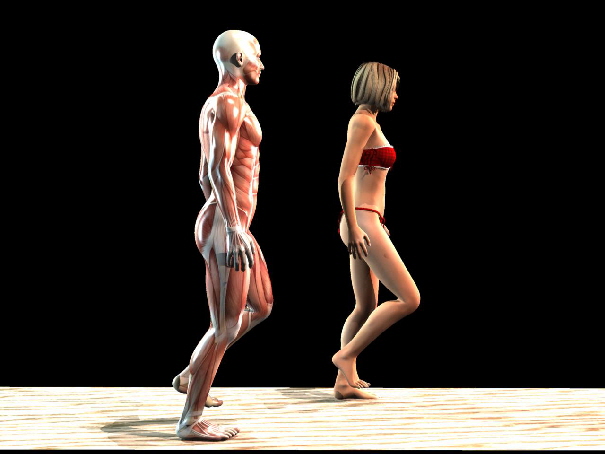
 As we grow from childhood to adults various things stop growing sooner. The big obvious difference between the
proportion of children to adults is indeed the center of mass. Kids are big bodies with short legs. Once they hit that teen spurt the body growth slows then stops and we get remaining growth from
the legs alone. In another way of looking at it, sitting height in young teenagers is nearly normal adult height. But as the legs grow standing height gains the advantage.
As we grow from childhood to adults various things stop growing sooner. The big obvious difference between the
proportion of children to adults is indeed the center of mass. Kids are big bodies with short legs. Once they hit that teen spurt the body growth slows then stops and we get remaining growth from
the legs alone. In another way of looking at it, sitting height in young teenagers is nearly normal adult height. But as the legs grow standing height gains the advantage.


 |
|||||||||||||||
|
|
|||||||||||||||