Ponseti Method
of Treatment of Club Feet
One method of treatment stands out for several reasons. Professor Ponseti, of Iowa, has refocused attention on the "conservative" (usually a synonym for non operative) treatment of club foot. It had seemed as if that topic was dead and buried. Yes SOME feet CAN be well treated with casts (or very skilled daily manipulations - as in France) - but ?? ALL ?? non surgically?
The devil is in the details. Firstly the Ponseti method of foot manipulation is very well thought out and is the method we ourselves use and have used for quite some time for newborns. Assuming that this intervention begins very early, a very good inroad on hind-foot and mid foot repositioning ought to be attained.
But ALL of them? If I understood the professor correctly, on direct questioning, well obviously not those rock solid ones that don't budge - nothing touches those - the issue is the treatable ones, the ones that do budge...
OK. Now the stats seem to fall in line better, but there is still an impressive batting average that we who use that method can't seem to match. It's in the language. The professor is talking about the percentage of those feet that do budge who NEED THE BIG TAKE EVERYTHING APART OPERATION. Don't count that little early operation to lengthen the Achilles tendon... ahhhh, now the numbers fall in line, and they are still good - quite good.
So we are talking about a generality, a good one.
An example, given this club foot that has been systematically and methodically exercised
 |
and manipulated such that the shape of the foot seems right and the heel is better aligned relative to the ankle bone, but, at 6 months old the whole affair still is far from square with a floor standing posture... Then what? The big operation?
 A tiny outpatient (no need to stay in the hospital) lengthening of the more restrictive tethering of the heel achieves the desired goal and avoids the bigger surgery. It can be done with local
anesthesia. However, there can still be some residual offset that persists or which might recur with time. Aftercare is very important - in all methods. Bracing and exercises still go on.
Club foot seeks the club posture through growth even when "corrected".
A tiny outpatient (no need to stay in the hospital) lengthening of the more restrictive tethering of the heel achieves the desired goal and avoids the bigger surgery. It can be done with local
anesthesia. However, there can still be some residual offset that persists or which might recur with time. Aftercare is very important - in all methods. Bracing and exercises still go on.
Club foot seeks the club posture through growth even when "corrected".
 |
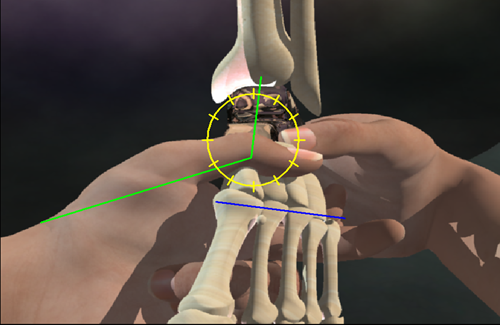
The essence of Ponseti manipulation is to move the entire foot around the talus. You have to hold the talus against the maneuver (here, the right thumb stabilizes the talus as the left hand moves the forefoot as a single unit around. The right hand index finger is helping the left hand by pulling the heel bone under the talus so as to stay with the mid foot. The heel bone has to both turn on a vertical axis and rotate on a horizontal axis. Got that? Good. But just in case you are not sure, I made this movie to help you visualize. It has a catchy tune as well and lyrics to help you remember.
|
The folks at Texas Scottish Rite also used Botox to soften another of the more resisting muscles. With such tricks we can avoid doing huge surgeries as a routine, but not as a guarantee. There still exists that pesky sub group. Some of those cases actually have bone bridging the deformity and are better placed in the category called arthrogryposis.
But if the smaller operation does not guarantee a full correction, why try? Because when it works, and it usually does, the foot QUALITY is better. The surgically "corrected" feet are not functionally equivalent to normal feet in terms of controlled supple range. One of the problems with the data is that sources differ in so many ways. Special incisions were heralded as allowing "better" exposure for more complete correction. With that came a percentage of cases with diminished luster from overshoot. They're not bad, but they're not as pretty as some others.
We consider the Ponseti method the replacement for the "Kite" standard that had been the gold standard of "conservative" club foot care. The Kite method had a success rate of about 40% if success only means no need for surgery under anesthesia. Interestingly, that method frequently employed anesthesia or advanced sedation in the manipulation and cast application - many times. The failures were not disasters, just that surgery was needed as well. That surgery was easier as a result of the treatment.
The Turco advance in surgical methods actually allowed the consideration of good outcomes in the vast majority of cases, given the conservative treatment that set the stage for its implementation at about 8 months to 1 year old.
The Ponseti method brings many more cases into the conservative fold if you can live with the small procedure done in the very early phase as still being a part of "conservative care". It has excellent characteristics of its end product. Just know that the percentages quoted by various authors are not addressed in equal terms and are flat out confusing.
Did this help?