
AFO Examples
There are so many kinds of ankle-foot orthoses (orthosis = brace) that it is easy to get mired in extraneous detail. Let's look at examples
just to ground ourselves in tactile realities. First the bad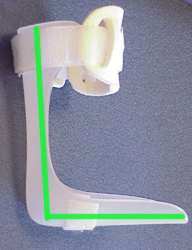 :
:
This is what we call a landfill orthosis. Depending on the child's need, braces can do various things. It is hard to imagine just what this brace can do well. It is formless, lacking fit detail. Most likely, it is one of those one size fits many (off-the-shelf) items. A minimum requirement would be to hold at least 90 degrees (allowing for an appreciable shoe heel height). If a flat sneaker were worn, then this brace lacks sufficient forward tilt for even standing (which requires 10 degrees forward tilt - in the shoe - for balance). It does not cover the ankle bones, and therefore is very unlikely to control left-right ankle sway. It will not correct nor prevent flat foot or varus (club-like) posture. The foot side portions protrude too far forward. That extra extension of inadequate sides simply prevents flexibility at the metatarsal heads (ball of the foot, just behind the toes). Forward roll is killed. The forefoot "trapping" caused by this defect will cause the foot to spin on the stuck toe area into excess inward or outward leg rotation, whichever is easiest. This brace causes malrotation in late stance phase as the leg tries to swing impeded by the stuck toe area.
The backward lean of this brace will cause the child to flex at the hips to balance the body weight over the feet. This "jack knife" hip posture is often blamed on torso or hip weakness.
 Here are two kinds of AFO that do meet all the requirements. These are commercial products, ordered from afar, but fit based on a local vendor heeding the
important details. Beware, although we are showing them as optimum examples, poor ordering and fitting skills can mess them enough to be useless. On the left, are front and side views of solid ankle AFOs. On the right, the side view of a hinged AFO.
Here are two kinds of AFO that do meet all the requirements. These are commercial products, ordered from afar, but fit based on a local vendor heeding the
important details. Beware, although we are showing them as optimum examples, poor ordering and fitting skills can mess them enough to be useless. On the left, are front and side views of solid ankle AFOs. On the right, the side view of a hinged AFO.
The SOLID AFO:
Well shaped to the foot, flexible fit with full contact padding at key pressure points. Ball of foot toe-plate area is flexible and not bounded by sides that would impede toe roll over. The vertical
10 degree forward pitch is perfect, especially for sneaker wearing. There is sufficient strapping and forward ankle envelopment to keep the foot shaped and positioned where intended. Remember, there are two main objectives. 1) Walking and 2) Shaping the foot against deformity.
If the latter is important, then the enveloping fit, as seen here, is ideal. The main problem with this orthosis, is that there are certain kids with postures that simply cannot attain this ideal
configuration. They need totally custom fit orthoses that, by application of filler material (applied outside the brace), the brace attains an outer contour that looks like this even though the ankle
and foot, inside, do not. Thus we satisfy an inner anatomy shaping-holding need as well as the outer walking geometry. We marry the concepts of orthosis making with prosthesis making.
The HINGED AFO:
Some children have mostly foot shaping needs. Hinges are fine, in that case. However, some have control only so far and not with every step. Rather than allow any degree of free forward movement, a back strap is used (see image) which lets the brace go so far and no further. This is
a "control arc" concept. Allow some range which has demonstrated control (strength equal to the task and reaction speed), but no more. Range without control is, well, you know.
The SPIRAL AFO: Another way to allow "control arc" (limited arc) motion
in ALL directions (not just forward) and even nudge in one particular direction, is the spiral AFO. Certain children almost demand these. Regardless of the medical biomechanical logic or physical needs, the athetoid
patients, ataxic patients, and some dystonic patients fall apart when held stiffly. In these sensory dependent conditions, DAMPENING motion beyond an allowed minimum is better than complete limitation. The spiral
fit allows flexibility, the carbon component, limits or encourages motion in one direction over another. Because these cases are so sensory needy,
leaving the ball of the foot and toes uncovered is best (tactile reasons, not brace reasons). In fact, the strategy is to see how little covering can hold all the anatomical requirements and also to see
how thin (for sensory reasons) the brace bottom can be without the brace falling apart. These orthoses work when others fail. Down side? They are beasts to make and worse to adjust. Those
few brace makers who can make this brace, groan when they are asked to do so.
Another way to allow "control arc" (limited arc) motion
in ALL directions (not just forward) and even nudge in one particular direction, is the spiral AFO. Certain children almost demand these. Regardless of the medical biomechanical logic or physical needs, the athetoid
patients, ataxic patients, and some dystonic patients fall apart when held stiffly. In these sensory dependent conditions, DAMPENING motion beyond an allowed minimum is better than complete limitation. The spiral
fit allows flexibility, the carbon component, limits or encourages motion in one direction over another. Because these cases are so sensory needy,
leaving the ball of the foot and toes uncovered is best (tactile reasons, not brace reasons). In fact, the strategy is to see how little covering can hold all the anatomical requirements and also to see
how thin (for sensory reasons) the brace bottom can be without the brace falling apart. These orthoses work when others fail. Down side? They are beasts to make and worse to adjust. Those
few brace makers who can make this brace, groan when they are asked to do so.
Combination Needs: Some children have foot needs met by their AFOs, but that alone does
not control a remaining problem, leg rotation. A twister cable (metal cable) or a side metal bar extending down from a metal or plastic pelvic piece can satisfy that. But a simple elastic strap, as shown on the right,
attached by Velcro to a neoprene pelvic belt also does fine. Structurally, elastic control straps are like garters with an attitude. Parents can easily adjust the latter and use them intermittently as need requires. The
elastics are soft, cheap, and easily modified. Strung as shown, they let go (pull wise) in sitting. If the straps are run deep to the underpants, then the
kids can toilet without somebody helping. They hide well. Elastics work best attached high, that is, at the top of an AFO. Hooked to a shoe, without some kind of ankle
area hold, , they MIGHT just twist the foot more so than the leg.
Some children have foot needs met by their AFOs, but that alone does
not control a remaining problem, leg rotation. A twister cable (metal cable) or a side metal bar extending down from a metal or plastic pelvic piece can satisfy that. But a simple elastic strap, as shown on the right,
attached by Velcro to a neoprene pelvic belt also does fine. Structurally, elastic control straps are like garters with an attitude. Parents can easily adjust the latter and use them intermittently as need requires. The
elastics are soft, cheap, and easily modified. Strung as shown, they let go (pull wise) in sitting. If the straps are run deep to the underpants, then the
kids can toilet without somebody helping. They hide well. Elastics work best attached high, that is, at the top of an AFO. Hooked to a shoe, without some kind of ankle
area hold, , they MIGHT just twist the foot more so than the leg.
 When knee protection is required, a thigh cuff is added (left). If the hinge at
the knee is unlocked, the thigh cuff does virtually nothing to walking. It is merely good protection of the knee against side to side forces. This is
especially important in children with spina bifida. They can actually destroy the knee joint before their teen years if the knee lacks such protection (as they have unique muscle instability problems at the knee).
When knee protection is required, a thigh cuff is added (left). If the hinge at
the knee is unlocked, the thigh cuff does virtually nothing to walking. It is merely good protection of the knee against side to side forces. This is
especially important in children with spina bifida. They can actually destroy the knee joint before their teen years if the knee lacks such protection (as they have unique muscle instability problems at the knee).
Also at the left, we see another control arc solution at the ankle. The hinge
has two set pins within it (occasionally with springs). They can be set to allow so much foot pointing up and also set so much foot pointing down.
Although such hinges are classically attached directly to the shoe, modern construction also allows a molded plastic foot orthosis to be inside the shoe as the attachment, as shown here. This
image also shows the use of leather (stiffened by shaped metal stays) as an alternative to plastic. Why? Better pressure properties for insensitive skin and better breathing for circumstances of
excessive sweating. Some of the most "impossible" to brace kids who suffer skin breakdown will thrive in these.
 Bracing primarily for deformity means getting out of the way of
functional motion and both holding enough body to have sufficient push and to have enough square inches to dissipate those forces. Skin breaks down if focal pressure exceeds 7 pounds per square inches. If you need,
say, 20 pounds of push to reshape a limb contour over time, you had better have more than 3 square inches of contact at the push area. Do the math. Add to that, impulse loading (kids jump a lot).
Bracing primarily for deformity means getting out of the way of
functional motion and both holding enough body to have sufficient push and to have enough square inches to dissipate those forces. Skin breaks down if focal pressure exceeds 7 pounds per square inches. If you need,
say, 20 pounds of push to reshape a limb contour over time, you had better have more than 3 square inches of contact at the push area. Do the math. Add to that, impulse loading (kids jump a lot).
So, for Blount's disease, for example, we do not need to worry about
control arcs, as the kids are totally normal in skills. We need to change shape, the leg angles AND twists. Twisting is easier when the joints are bent (eg: knee flexed). Alignment angles of the long bones are most
efficiently steered when the limbs are straight (extended). Such braces allow full ranges to get at both postures (as the child moves). The same brace corrects different
parts of the problem as the child moves into different positions.
Add to that, that there is no way to just push the leg totally straight in one oomph. It will break
the leg to "correct" it all at once. The brace must be made, initially, in the shape of the deformity then gradually recontoured every so many weeks to allow the anatomy to biologically reshape by
way of its growth. Unless the child has unusually slow growth milestones, this gets to be quite difficult by age three. That means we have to be about DONE by age three. That, in turn, means
that we have to identify the ones who should be braced EARLY and just get on with it. You CAN think this to death.
There are two ways to identify the brace needy group. 1) The lazy way, let all those who will get better (physiologic bowing) get better and whoever is left must be the ones. Or, 2) actually look closely. Physiologic bow is usually minimal with actual bow shape minimal to zero, most being twist (torsion). The physiologic ones are improving with time. Blount's disease has major high tibial angulation with a few other oddities, and twist as well. The big thing is that Blount's kids are WORSENING (even at 18 months old, worsening is NOT physiologic). An x-ray taken with the knee pointed straight ahead (foot looks wrong when doing it correctly) will show that a line (weight bearing line) drawn on the x-ray from hip to ankle passes outside the knee - unsupported by bone. That lack of support may very well be what pinches and damages the inner growth plate at the knee to create Blount's disease (or at least what makes it become a permanent growth defect, rather than a passing phase).
What does this have to do with AFOs? Well, the AFO may actually get in the way. These braces need special metallurgy for the reshaping and AFO components may overly stiffen the construct creating too high a focal pressure at the knee. See?